
The SWEET programme has developed and completed feasibility testing of the HT&Me support package. The randomised controlled trial to investigate the effectiveness of HT&Me in reducing poor adherence to hormone therapy and improving quality of life in women with early breast cancer is now closed. The HT&Me support package included:
- A short animation video explaining how hormone therapy works, why it is important to take daily, and advice for managing side-effects
- Two appointments with HT&Me Study Nurses/Practitioners
- Access to the interactive HT&Me website, accessible on a desktop computer, laptop computer, tablet or mobile phone
- Regular text or email messages reminding of the importance of hormone therapy and signposting back to the HT&Me website
Recruitment for the study is now closed. We recruited a total of 1676 women who were randomised to receive either:
i) the HT&Me support package alongside their usual care
or
ii) usual care alone
Women were asked to complete a questionnaire when they signed up to the study (baseline), and then again 6,12 and 18-months later. These questionnaires will measure adherence to hormone therapy, quality of life, and other factors that might impact the effectiveness of the HT&Me support package.
To read about our earlier intervention development work click here and feasibility study click here
We are also conducting a cost-effectiveness evaluation and developing a scale-up implementation strategy, to read about these please click on the workstreams below.

The programme includes five workstreams, as shown below.

Workstream 1 involved the design, development and optimisation of the HT&Me support package. It was developed using an evidence-based and theory-informed approach. Patient and public involvement (PPI) has been integral to all stages of design and development.
Within this workstream we conducted two optimisation studies to collect user feedback. This informed improvements to the HT&Me support package. Preliminary data suggests the HT&Me support package is acceptable and engaging to users.
The diagram below provides an overview of the support package development, design and optimisation process.
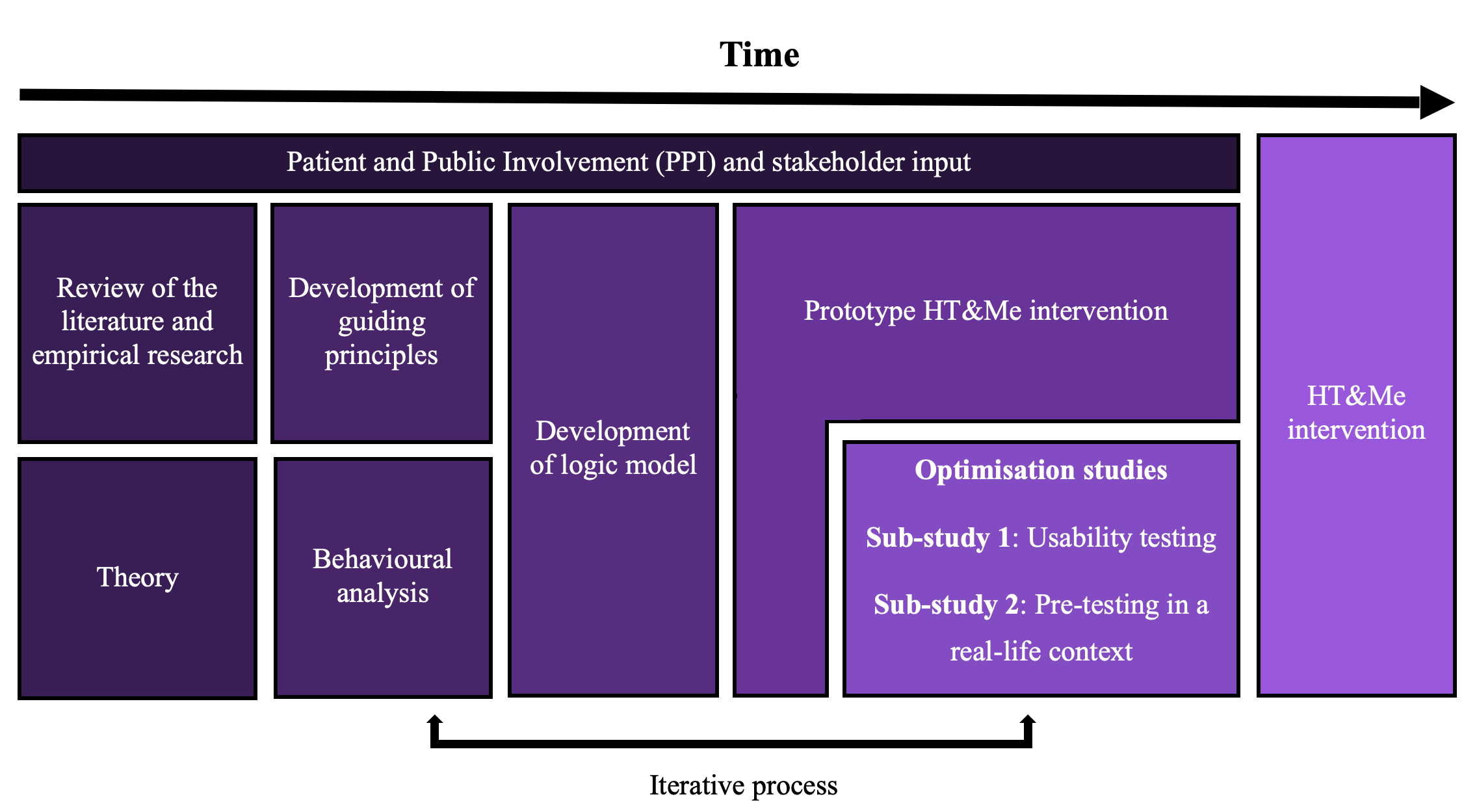
Workstream 1 is complete, and the development process has been published: click here
Workstream 2 assesses the feasibility of the HT&Me support package for both users and healthcare professionals, across two sub-studies. To do this, we have recruited 59 women who had been prescribed hormone therapy for early breast cancer across 5 NHS sites in England to our first sub-study. Women received the HT&Me support package for 8 weeks alongside their usual care and completed a questionnaire before they received the support package, and then a second one 8 weeks later. We interviewed 20 of these women to hear about their experiences of the HT&Me support package. We also interviewed 13 of the key healthcare professionals that were involved in delivering the support package across our sites to gather feedback on the study processes. Data has been useful to inform the randomised control trial (RCT) (Workstream 3).
In a second sub-study, where 56 women were recruited, we have tested the feasibility of accessing, and analysing, prescription encashment and GP prescribing data to objectively measure adherence to hormone therapy.
We have recruited women from the following sites:
- Gateshead Health NHS Foundation Trust
- Great Western Hospitals NHS Foundation Trust
- Imperial College Hospital Trust
- Newcastle-upon-Tyne Hospitals NHS Foundation Trust
- Oxford University Hospitals NHS Foundation Trust
Workstream 2 is complete, and the findings have been published, to read them click here
The SWEET Feasibility data controller is Newcastle upon Tyne Hospitals NHS Foundation Trust (NuTH)
Privacy notice: click here
To email for Data Protection Officer at NuTH:
- Email: nuth.dpo@nhs.net
The SWEET Feasibility data processor is Newcastle University
Data protection policy at Newcastle University: click here
For more info on how we use your information, click here
For a link to the information commissioner’s office, click here
To email for patient relations (NuTH):
Workstream 3 involves the delivery of a randomised control trial (RCT) alongside a process evaluation. Recruitment has now closed and we are in the follow-up stage.
We are investigating whether the HT&Me support package improves adherence to hormone therapy and cancer-specific health-related quality of life.
To do this, a total of 1676 women with early breast cancer were randomised to receive
i) either the HT&Me support package alongside their usual care,
or
ii) usual care alone. Women were asked to complete questionnaires when they signed up to the study (baseline), and then 6, 12 and 18-months later. These will measure their adherence to hormone therapy, quality of life, and other additional factors that might impact the effectiveness of the HT&Me support package.
Watch our video below on how to navigate around the HT&Me website.
In Workstream 4, we will look at what HT&Me costs compared with usual NHS care and whether it is good value for money compared with other services the NHS could spend money on. We are collecting data on trial participants’ quality of life, what NHS healthcare they use and any costs to them or their families arising from breast cancer. We will estimate the cost-effectiveness of HT&Me in terms of the cost per healthy year (Quality Adjusted Life Year “QALY”). We will also estimate the total cost of the implementing the HT&Me programme to the NHS. Our main analysis will look at results for all trial participants up to the end of the trial, but we will also do other analyses to explore how costs and benefits might change in the future. We will use the same methods as UK policy-makers, such as NICE, so that the evidence from the trial can feed into NHS decisions.
The aim of Workstream 5 in the SWEET programme is to develop a pathway to impact and inform potential scale-up across the NHS.
Workstream 5 objectives are to use a combination of theory, qualitative research and stakeholder involvement to:
- understand and articulate the context and complexity of the intervention (HT&Me) in order to inform its implementation and scalability across the NHS
- maximise the potential impact of the research programme for patients, healthcare professionals and other key stakeholders.
An implementation strategy is a ‘how to’ plan for ensuring that an intervention is adopted and sustained. We have utilised the initial phases of the EPIS framework (Exploration, Preparation, Implementation, Sustainment) as a guide click here. The implementation and sustainment phases of this framework will only be relevant during and following implementation of HT&Me into routine practice.
In the exploration phase, we worked with our Patient Advisory Group (PAG) and Clinical Reference Group (CRG) to develop the intervention (HT&Me), based on the best current evidence, to ensure that it had the best chance of being implemented successfully within an NHS context. To read our paper on the development of HT&Me click here. One of the key considerations of this phase was enabling flexibility of intervention delivery: through for example two models of consultation (hospital site breast cancer team or remote delivery via specialist nurses at Breast Cancer Now), a modular training resource and an interactive website for patient participants.
In the preparation phase, we have focussed on two key areas:
• Gaining internal and external support for HT&Me, which has involved regular communication with clinical and research staff within our trial sites as well as with our key charity partner, Breast Cancer Now. We have liaised with many other groups and organisations, including cancer alliances, health innovation networks, professional organisations such as the Association of Breast Cancer Surgeons and patient-facing information organisations such as patient.info. We have presented HT&Me to multiple groups, including Breast Cancer Now webinars, Primary Care networks and professional conferences.
• Identifying key implementation challenges through our process evaluation involving interviews with women and healthcare professionals, and through a survey of our participating sites, in which we have asked clinical teams about the support they routinely provide for women with breast cancer who are on adjuvant endocrine therapy and about their views of the intervention and how it might be implemented beyond the trial.
In all this work, we have mapped contextual and intervention-related factors that are likely to influence implementation to the constructs specified within the EPIS framework. These are described as:-
Outer Context: NHS and policy environment, Funding, National leadership and support, Patient population, needs and characteristics, Patient advocacy factors.
Inner Context: organisational characteristics, leadership within organisations, staff characteristics, quality and fidelity.
Innovation factors: how HT&Me ‘fits’ into the existing system, how easily it can be adopted.
Bridging factors: partnerships that can facilitate implementation and adoption.
 1. SWEET-PLUS: Supporting adherence to adjuvant CDK4/6 inhibitors in women with early breast cancer
1. SWEET-PLUS: Supporting adherence to adjuvant CDK4/6 inhibitors in women with early breast cancer
Background
Breast cancer is the commonest cancer in UK women. While many women are diagnosed with early-stage disease, meaning the cancer hasn’t spread, there is still a risk the cancer could come back (recur), even after successful hospital treatment. For women whose cancers are sensitive to the hormone oestrogen, doctors recommend hormone therapy for 5-10 years after hospital treatment to reduce the chance of recurrence.
New drugs – called CDK4/6 inhibitors - are now being used alongside hormone therapy to further reduce the chance of the cancer coming back. However, studies have shown that many women stop taking these drugs before the two or three year recommended treatment period. Not following the treatment plan could mean the drugs don’t work as well. To get full benefit of these new drugs, women should be supported to take them as recommended, wherever possible.
Aims
This SWEET-PLUS project will understand what helps, and what makes it difficult, for women with early breast cancer, who are prescribed CDK4/6 inhibitors, to keep taking them as recommended. Using this information, we will create a support tool, in collaboration with patients, that will help women take their treatment as recommended.
Design and methods
SWEET-PLUS will have three phases:
Phase 1: We will interview around 25 women with early breast cancer who use or have used CDK4/6 inhibitors to learn about their experiences. This will help us understand what challenges they face, how they feel about taking the drug every day, and what might help them stick to the treatment plan.
Phase 2: We will also hold focus groups with around 20 healthcare professionals, including doctors and nurses, to understand how they prescribe CDK4/6 inhibitors and what advice they give women about continuing or stopping early.
Phase 3: Using insights from women and healthcare professionals, we will work together to develop a support tool to help women take their CDK4/6 inhibitor as recommended. This will be an addition to our existing HT&Me support package which we developed to help women stay on hormone therapy. We will look for more funding to test the new tool.
Public & Patient Involvement
Women with breast cancer and experience of CDK4/6 inhibitors have been involved in developing the project and will continue to play a key role throughout. They will help design patient materials, advise on recruitment, review results, and co-develop the support tool.
Impact and Dissemination
Our support tool will help women take their treatment as recommended, which will ultimately reduce the chances of the cancer returning and improve survival rates. This will benefit patients, their families, and the NHS. We will share results in papers, briefings and infographics and work with charities and other organisations to ensure they are used to benefit patients.

2. QUIETER+ Inequalities in adherence to endocrine therapy in women with ER+ve breast cancer: can these explain disparities in survival?
Background
In the UK, women with breast cancer living in more deprived areas, and Black women, have shorter survival. We don’t understand why. One reason could be differences in treatments between different groups of women. Endocrine therapy (ET) is recommended after surgery for oestrogen-receptor positive (ER+ve) breast cancer. By controlling levels of the hormone oestrogen in the body, it reduces the risk of breast cancer coming back (recurrence) and of dying. It is taken as one tablet every day, for at least 5 years. However, up to half of women regularly miss ET tablets (accidentally or deliberately) or stop taking ET completely. This increases their chance of dying from breast cancer. Studies in other countries suggest women from deprived communities and Black women are more likely to miss or stop their ET. We think this may be an important contributing factor to the shorter survival seen in these groups of women.
Aims
First, we will investigate if there are differences in the amount of ET women with breast cancer in the UK (known as “adherence”) according to where they live (deprived areas vs. affluent areas) and their ethnicity. Second, we will find out whether differences in the amount of ET taken can explain differences in survival by deprivation and ethnicity.
Methods
We will use data from the Clinical Practice Research Datalink, a collection of people’s GP records. This will be “linked” to other NHS datasets to find out who developed cancer, and who died and when. Our study will include around 35,000 women with breast cancer, diagnosed January 2005-December 2019, who had at least one ET prescription after surgery. For each woman we will look at her prescriptions to work out whether she (1) continued, or stopped, taking ET and (2) missed ET tablets; these two things measure adherence. We will compare adherence across deprivation and ethnic groups. We will examine whether adherence is related to cancer recurrence and survival. Then, we will investigate how women’s deprivation level, ethnic group, adherence and survival are related – whether differences in adherence between groups can explain differences in survival.
Potential impact
This project will help understand where action is needed to reduce survival differences. For example, if we show that lower ET adherence is a reason why more deprived and ethnic minority women have lower survival, this will mean these groups might benefit from more support with taking ET. This could help improve breast cancer survival, benefiting patients and the NHS.